

Is polyvagal theory the educated progressive's colloidal silver?
Stephen Porges, if you're reading this I'm so sorry!

Dr. Stephen Porges, the daddy of polyvagal theory, has published on the vagal nerve since the 90s, but the 2010s were the decade of the polyvagal theory1 explosion in psychotherapy.
I’d heard about fight and flight responses or and the different nervous system branches before college. It’s fairly common knowledge that in times of stress, we automatically shift into a different state and engage in physiologically useful behaviors without conscious effort.
By the time I got to graduate school in 2016, polyvagal theory was all the rage. The Body Keeps the Score came out in 2014. There was nothing sexier than remembering the structures and functions of the nervous system. Being the first person in your class to mention the freeze response, or better yet, a dorsal vagal shutdown, was the best way to distinguish yourself from the not-trauma-informed losers. Somatic therapies were in high demand and CBT was for idiots.
I thought I was fundamentally unintelligent because I couldn’t memorize it. I went to trainings, I drew diagrams, I read books and blogs. Notably, all secondary sources. I remembered learning about the vagus nerve in behavioral neuroscience class in college, but it had been a while and I was always sleepy cause that class was after lunch. I remembered the basics, and I shared the basics. In grad school, I tried to catch up with my apparently huge-brained peers. I had images saved to my desktop so I could quickly print them and pass them on to my clients. And it was extremely useful! Those of us plugged into this therapeutic movement either through education or our own therapy learned to better listen to our bodies and soothe our nervous systems. The knowledge I personally gained through the work of Porge’s and his disciples is invaluable to me as a human being. But there was so much I could not absorb. I beat myself up for having questions I was too afraid to ask, because my classmates and colleagues seemed so sure.
But then, I was also sure that some of this was not adding up. I don’t remember the first time I heard the term “fawn response”, but that piece, for example, didn’t line up with research I had swallowed and regurgitated. I had only ever seen it described in terms of behavioral patterns emerging from conditioning when the whole point of the autonomic nervous system is the autonomic part. And I couldn’t ignore the fact that some of the people speaking authoritatively about mammalian nervous system evolution also made videos about adrenal fatigue.
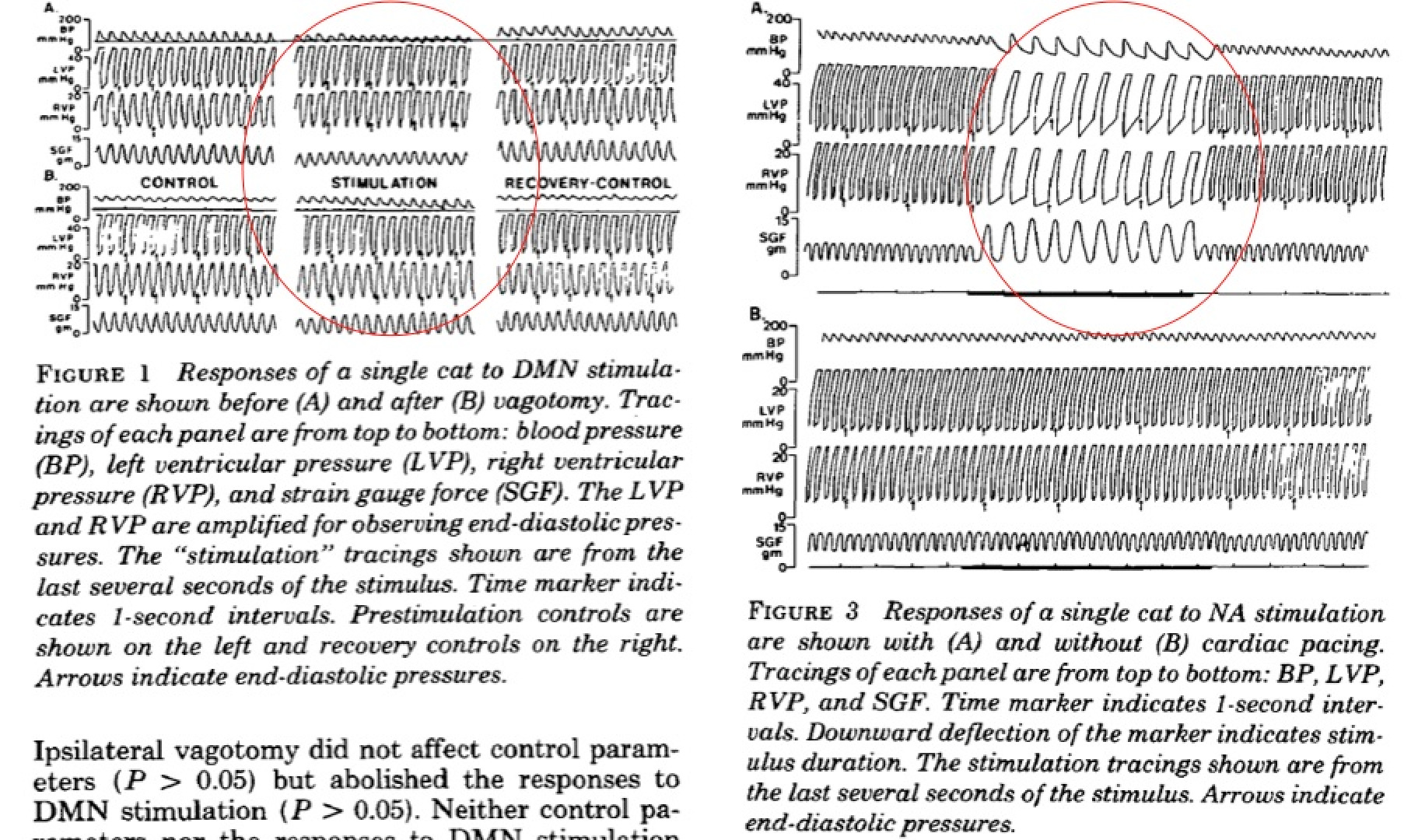
I began to crack into the primary sources. But look. I know where I belong, and it sure as hell isn’t journals called “Comprehensive Psychoneuroendocrinology”. I could read the words vagal preganglionic neurons and tell you what each one means, but that’s about as far as I get. What I did learn in these papers was that some hypotheses of polyvagal theory are testable, and they have not exactly held up. There are many critics in the scientific community, just none in the trauma-informed clinical social work world I belong to. The Polyvagal Institute assures me that criticism is misguided, that “Although hypotheses generated from Polyvagal Theory can be tested using respiratory sinus arrhythmia as an accurate measure of cardiac vagal tone, Polyvagal Theory is not based on respiratory sinus arrhythmia being an accurate index of cardiac vagal tone” and I shouldn’t worry about it. Uh, checkmate?
So how can I honestly endorse or criticize polyvagal theory, without a background in biology, psychiatry, neuroscience?
And that’s the whole point. I’m not equipped to evaluate the claims of the science of polyvagal theory, and neither are most people, including clinicians. I happened to have recent memories of behavioral neuro class. Many of us come to a master’s program with like, a BA in Spanish from 2007. Which is fine! But it makes us vulnerable to scientific misinformation in the classroom.
In college, I worked in the Chicago Lab of Emotion and Physiology with graduate PhD students who said mostly words I’d never heard in my life. I would trust them talking neuroscience with clients. I know there are scientifically inclined clinicians who can grasp this stuff. But honestly, that knowing is based on vibes. On an individual level, you could ask people about the classes they took, look at their credentials, check out papers they’ve co-authored, speak with their colleagues, and at least get a sense of what they know they don’t know. On the scale of the whole field of clinical psychology, we have absolutely no way of telling scientific practitioners from charlatans. And your average client doesn’t even know a CADC from an LSW from a PsyD.
If we’re going to engage in worship, why not chose scripture with easier-to-remember words? Fewer charts? First, the simplified explanation of polyvagal theory is just so damn lovely.
It’s a beautiful metaphor. An important function of therapy is meaning-making, especially in the presence of trauma. We have a need to create a new narrative about what happened that does not produce shame. Our bodies are trying to keep us safe all of the time, doing things outside of our consciousness to keep us out of harm’s way. We aren’t stupid for not fighting back against an attacker or running away from a loving embrace. We are doing exactly what we are supposed to do to survive. This is something every person deserves to hear.
But without a willingness to critique the model, we have no basis to reckon with the new-agey high-end market of polyvagal theory influencers. Though some openly believe in self-healing and discourage treatment, more responsible Instagram therapists/coaches/wellness instructors disclaim that their page/website/courses are just for education. But they’re not doing science communications, they’re evangelizing from the pulpit. And misapplying this theory can lead to bizarre and disastrous consequences: cutting important people out of your life simply because they “feel” “unsafe”, discontinuing helpful medication, blaming people in tough situations for not “doing the work” and ultimately, giving these grifters all your money.
But there are other factors fueling the polyvagal theory fire. I think it makes us sound smart. I think we think it makes therapists sound like scientists. And in a world (and importantly, economic model) that values hard science over all other kinds of knowing, scientific professionalization is what psychotherapists have been searching for all along.
And I can’t stop wondering if the popularization of polyvagal theory and its self-help applications are bolstered by our inability to simply go to the doctor. American right-wing boomers have shown demonstrated the lengths we will go to keep ourselves safe and healthy in lieu of a positive relationship with the healthcare system. Bleach. On the less desperate, less obviously paranoid end of the spectrum, we have neighbors with copper bracelets to help with circulation, aunts taking turmeric pills for their migraines, dads turning of the wifi at night to reduce EMF radiation. We crave control of our bodies.
Because most of us don’t receive medical care, we have to become “experts” on our health ourselves. And simply put: we can’t. It’s obvious in a sales pitch for a class where you can learn to heal yourself by strengthening your vagal tone, but it’s there when you assume you’re sleeping in class and on the bus and when you get home because of stress-induced shut down, and never think to see a doctor about your extreme hypersomnia (a little self-disclosure for reading to the end). Maybe it starts when you can’t access a doctor who takes your concerns seriously or when you can’t afford to go to the ER. It happens slowly, over time. Ideas like polyvagal theory are so compelling because if we can just figure out the code, we can do it ourselves. After all, chronic migraines/IBD/joint pain/acne is caused by stress, isn’t it?
There’s a part of me that’s still terrified to publish this. What if I was right before and I’m just not as smart as everyone else? Or maybe everyone just watched a documentary no one told me about. Or I missed a podcast episode. Please, if you know that I’m deeply stupid and should never talk again, let me know. I really do want to hear the perspectives of other folks in the field. If you’re willing to share, I would love to know how you’ve experienced the polyvagal theory and the general LevineVanDerKolkPorges trauma revolution.
I’m aware that what I’m calling “polyvagal theory” is actually a mix of different variously validated scientific understandings of how our bodies engage with and synthesize psychological stress, and that’s kind of the point. As a field, we’re constantly confusing language and anecdotes because most of us aren’t scientists. Calling it all “polyvagal theory” is just another way I demonstrate the obfuscation of it all and my own little contribution to the obfuscation because I do not have the education to keep it all straight.
I agree with Helena on this one, you seem to be conflating two differentiated phenomena. Not being able to access health care/being healthcare avoidant because it is unaffordable, racist and sexist and therefore trying to take care of yourself using other tools at your disposal is not a polyvagal problem, its a larger systemic problem. If anyone tries to use polyvagal theory or any other type of healing modality to the exclusion of all other forms of care, again that is an individual problem informed by a broken health/social system, not a polyvagal problem. If an Instagram therapist claims that learning about polyvagal responses will completely solve all their clients problems, that's a BAD therapist, and has nothing to do with the efficacy of polyvagal narratives to help people make sense of their responses. As a burgeoning therapist myself, the first course in my Masters was on the biopsychosocial model, looking at our client holistically, helping to offer suggestions of what might be going on biologically alongside their mental health struggles, and referring them to medical treatment alongside any treatment we give. Again, anyone on or off the internet pushing any one theory or practice as a cure all is a problem, but that's not unique to polyvagal theory. Shaming people for choosing to not seek medical help in an absolutely abhorrent medical system is misguided, as is blaming polyvagal theory for being a "snake oil" cure all instead of targeting its misuse or abuse by individuals in positions of social or economic power.
I had initially gotten caught up in the hype but then encountered the in depth criticisms by Paul Grossman and other experts in mammalian evolutionary biology and realized I didn’t know enough to trust the claims made by polyvagal theory and that the original knowledge base about fight and flight are helpful and I didn’t need to invent and imagine a dorsal vagal response to help clients. I think we are often too quick to want some kind of formula to help clients when really the self-knowledge and self-exploration that emerges within the therapeutic relationship can create growth and change over time and there is no magic panacea to rush or skip that process. Healing, insight, taking ownership over one’s life, etc. won’t happen through oversimplified and catchy memes.